Created 2008.
Dermoscopy is useful to distinguish pigmented non-melanocytic lesions from benign and malignant melanocytic lesions. There are specific features that help to distinguish seborrhoeic keratosis from basal cell carcinoma and melanoma. However, the distinction is not always possible and it may be necessary to excise some clinically atypical but histologically benign lesions.
The ‘wobble sign’ may be useful to distinguish a papillomatous melanocytic naevus from a stable seborrhoeic keratosis.
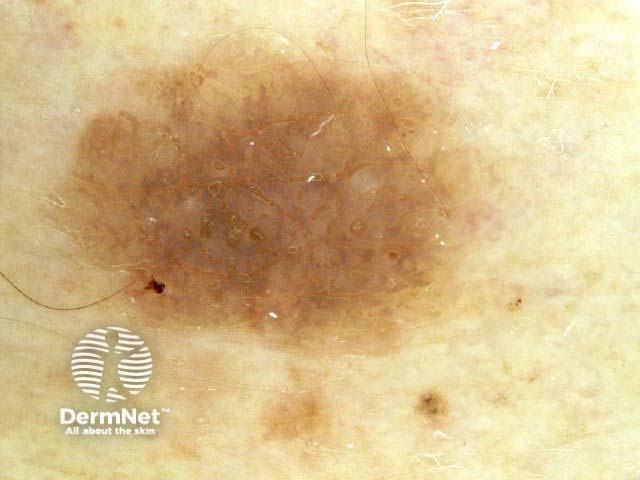
Seborrhoeic keratoses typically reveal dermoscopic features that are fairly specific for the diagnosis. However, on occasions, melanocytic lesions, especially dermal naevi, congenital naevi, Spitz naevi and nodular melanoma, may have similar features and can be just as difficult to distinguish from seborrhoeic keratoses by dermoscopy as clinically.
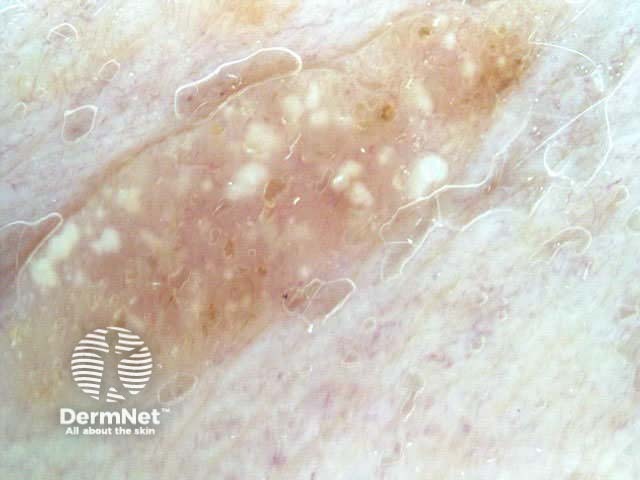
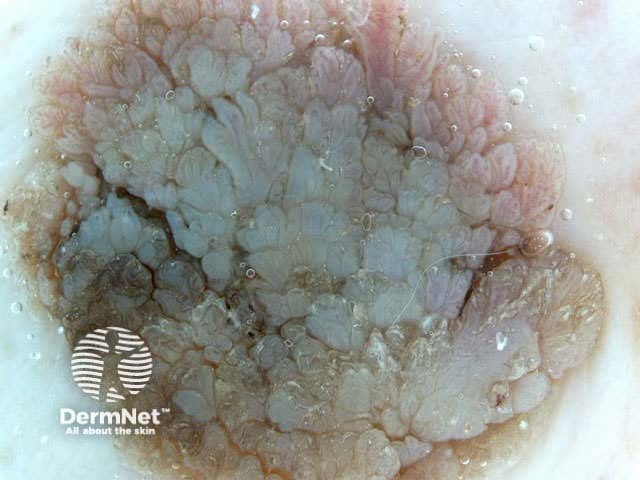
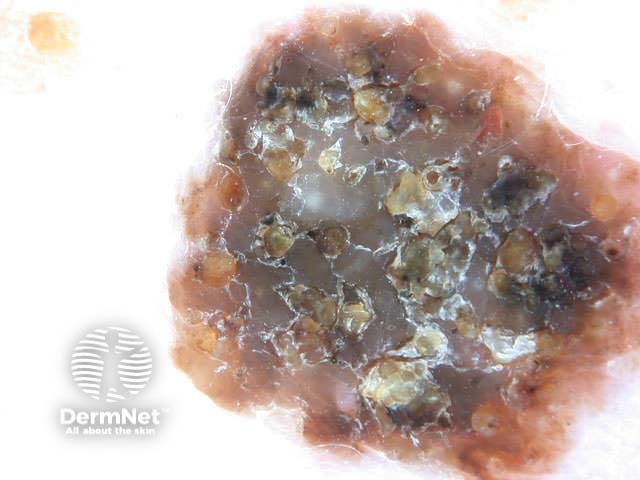
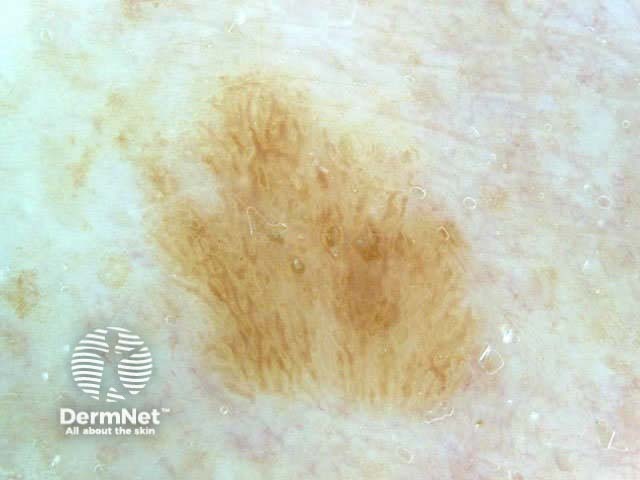
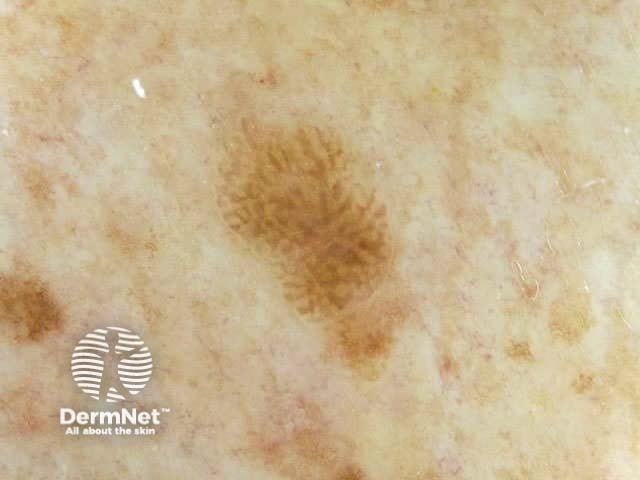
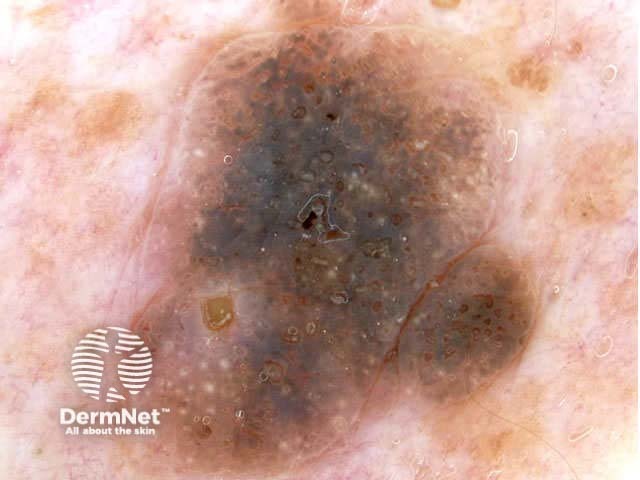
Seborrhoeic keratoses can have an irregular structure and multiple colours (skin coloured, pink, grey, yellow, tan, dark brown, black, bluish).
Typical dermoscopic features include:
There may also be a faint network or pseudonetwork. Blood vessels can be prominent in some seborrhoeic keratoses, tending to arise as tiny hairpin shaped capillaries surrounded by a halo within a lobule.

















Seborrhoeic keratoses demonstrate "chaos" by modified pattern analysis, ie, they often have asymmetry of colour and structure on dermatoscopy — like pigmented skin cancers. Clinical clues to seborrhoeic keratoses are:
Dermatoscopic clues to seborrhoeic keratoses by modified pattern analysis are:
If features are equivocal, excise the lesion. Partial biopsy may be acceptable if low-risk lesions, providing full excision is arranged should the atypical lesion prove to be melanocytic.
Evaluate 20 pigmented seborrhoeic keratoses by dermoscopy. What proportion contain each of the following features:
See the DermNet bookstore

